A lot of Georgia families reach this point after months, sometimes years, of steady progress. A teen is managing school, talking about a job, college, church, friends, and more independence. Then someone asks about driving, and the conversation changes fast.
For parents of teens with autism, ADHD, physical disabilities, hearing differences, a history of brain injury, or other support needs, the primary question is usually practical. Can this teen drive safely, and what is the right way to find out?
That question deserves a process, not a guess.
In practice, drivers ed for special needs students in Georgia works best when families treat driving as a readiness decision built on observation, screening, and the right instruction. Some teens do well on a standard permit path with more structure and more repetition. Some need a driving evaluation through occupational therapy before they spend much time behind the wheel. Some will need adaptive equipment, and that raises another set of decisions about cost, training, vehicle fit, and funding. Others may have the core ability to drive but are not ready for dense traffic, left turns across traffic, or the pace of metro Atlanta roads.
Licensure can be realistic for many teens with disabilities. The timeline is often different, and the path is rarely simple. In Georgia, the families who do best usually start by asking two grounded questions early: what skills are already present, and what barriers can be measured, trained, or supported?
Parents who want a broad overview of why formal instruction helps can review these benefits of driver's ed before choosing a program that fits their teen.
The Road to Independence Starts with a Question
A mother in Marietta once described this stage perfectly. Her son could memorize bus routes, follow routines, and talk for an hour about traffic signs. But when she imagined him making a left turn across busy traffic, she froze. That emotional split is common. You can see a teen's strengths clearly and still feel uneasy about the road.
Driving asks a lot from any beginner. It asks for attention, timing, judgment, emotional control, and physical coordination all at once. For a teen with special needs, the issue usually isn't desire. It's whether the instruction matches the way that teen processes information.
What families are really asking
Most parents aren't looking for false reassurance. They want a reliable way to answer a few practical questions:
- Can my teen manage multiple inputs at once? Road signs, mirrors, speed, pedestrians, and other drivers all compete for attention.
- Will anxiety shut the lesson down? Some teens learn well until traffic density rises or an unexpected event happens.
- Are we seeing a skill delay or just a training gap? Those aren't the same thing.
Practical rule: Don't treat hesitation as failure. Treat it as information.
When families rush past that distinction, they either push too hard or pull back too early. Both create problems. Pushing too hard can raise anxiety and make the car feel unsafe. Pulling back too early can prevent a capable teen from developing skills that would emerge with the right support.
A different map works better
The strongest programs for drivers ed for special needs learners don't assume that every student should learn in the same order, at the same pace, or with the same teaching method. They slow down the chain of skills. They separate scanning from steering, parking lot work from neighborhood driving, and traffic judgment from pure vehicle control.
That approach matters because the goal isn't just a license. The goal is durable independence. A teen who learns patiently and thoroughly is more likely to become a confident driver than a teen who gets pushed through standard lessons that never matched their needs in the first place.
Assessing Your Teen's Readiness to Drive
A parent usually knows the moment this question gets real. Your teen remembers routes, follows household routines, and asks for more independence. Then a crowded left turn, a sudden horn, or a change in plan reveals how much driving asks of attention, timing, judgment, and self-control all at once.
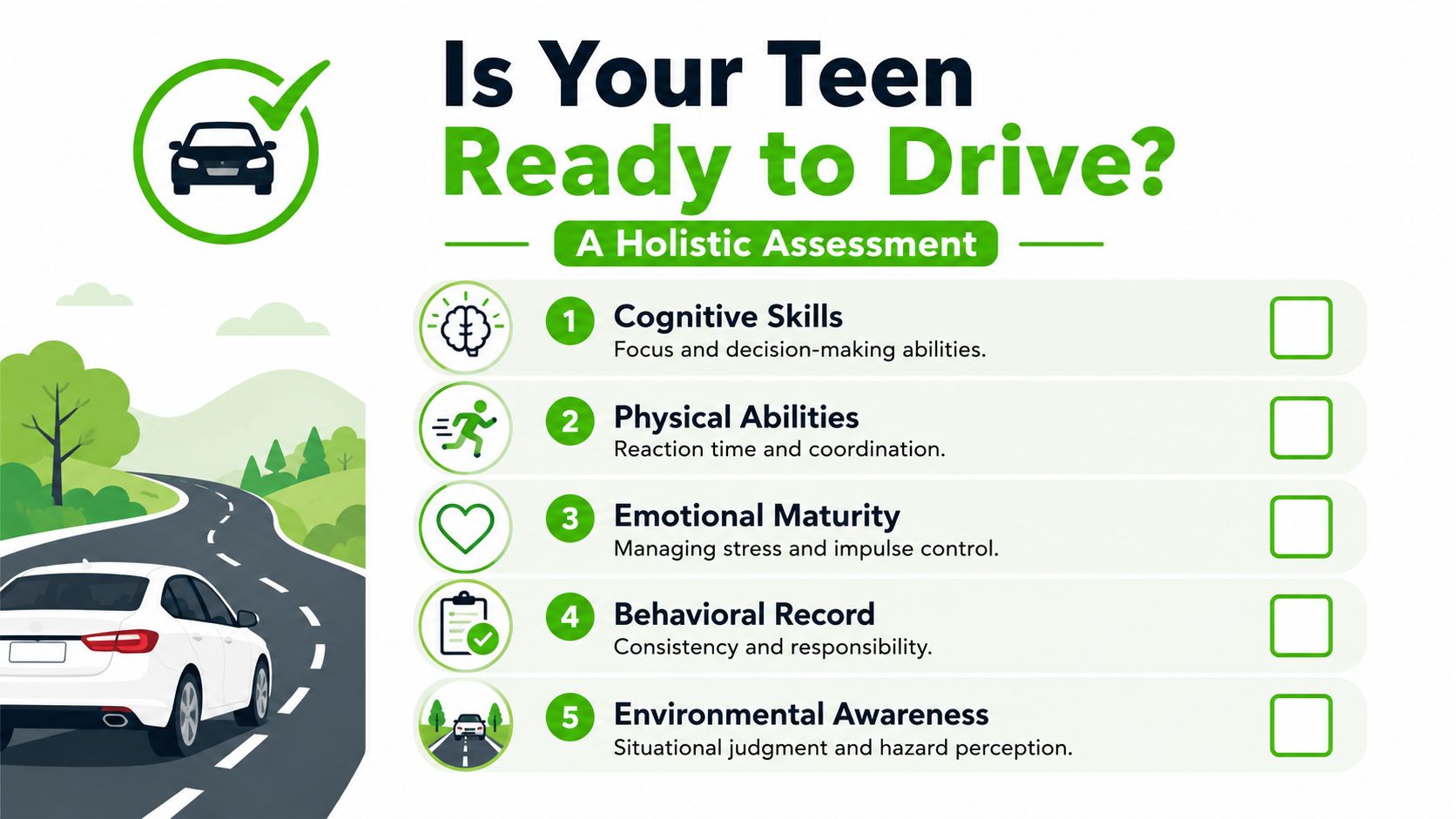
Readiness has to be judged as a set of skills, not a single trait. In practice, I look at five areas first: attention, regulation, visual processing, motor coordination, and follow-through outside the car. A teen does not need perfection in every area to begin. They do need a pattern of skills that can support safe learning.
That distinction saves families time and money. It also keeps them from paying for lessons that are premature, or delaying training for a teen who could do well with the right supports.
What to watch before you schedule road lessons
Home and school routines often give the clearest early signs. Look for consistency across weeks, not one unusually good day.
- Attention under load: Can your teen keep working when there is noise, conversation, or time pressure?
- Impulse control: Do they stop, check, and then act, or do they react first?
- Recovery after stress: After a mistake or surprise, can they regroup within a reasonable time?
- Visual scanning: Do they notice what is happening around them, or fixate on one detail and miss the rest?
- Motor planning and coordination: Can they sequence movements smoothly, including foot transitions, head turns, and steering control?
- Real-world responsibility: Medication routines, curfews, school tasks, and appointment follow-through matter because driving depends on reliability.
Parents can gather good observations here. A clinical driving evaluation adds something different. It tests the actual demands that tend to break down behind the wheel.
Why a formal evaluation is worth doing early
A strong OT or driver rehabilitation evaluation breaks readiness into measurable parts. Instead of asking whether a teen is ready in the abstract, it checks visual scanning, divided attention, processing speed, reaction time, executive function, and physical access to the vehicle. That gives families a clearer answer about what needs teaching, what needs accommodation, and what may need more time.
This is also where cost planning starts to become clearer. If a teen may need pedal extensions, hand controls, a spinner knob, left-foot acceleration, or transfer equipment later, identifying those needs early prevents wasted lessons in the wrong vehicle. In Georgia, that matters because adaptive instruction and vehicle modifications can become expensive fast. Families make better choices when readiness and equipment planning are considered together rather than as separate problems.
For teens with attention regulation concerns, outside reading on support for driving with ADHD can help families sort out whether distractibility looks manageable with structure, or whether it is still interfering with safe learning.
A good readiness evaluation should end with a training plan, accommodations to try, and a clear recommendation about whether to start now, wait, or begin with off-road skill building.
Readiness and permit eligibility are not the same
Georgia law sets the path for getting a permit. Functional readiness determines whether permit practice is productive and safe. A teen can be old enough and legally eligible, yet still need work on regulation, scanning, or motor coordination before regular road practice makes sense.
If you need the state steps, this guide on getting your learner's permit in Georgia covers the permit process clearly. Use that checklist for the legal side. Use a readiness assessment for the clinical and practical side.
Finding the Right Driving Program in Georgia
Once readiness is reasonably clear, the next fork in the road is choosing instruction. Often, many families lose time and money, because they enroll in a standard teen driving package when they really need adaptive instruction.

A traditional program often works well for typical beginners who need basic rules, supervised mileage, and ordinary correction. It usually doesn't work as well when the student needs sensory accommodations, task segmentation, adaptive controls, or a clinician who can interpret how a diagnosis affects road behavior.
Standard school versus adaptive program
A simple comparison helps.
| Program type | Best fit | Where it helps | Where it falls short |
|---|---|---|---|
| Standard driving school | Teens who learn with typical pacing | Permit prep, routine road practice, common maneuvers | Limited adaptation for cognitive, sensory, or physical differences |
| Adaptive driving program | Teens who need individualized pacing or equipment | Diagnostic teaching, custom strategies, readiness-based progression | May require more coordination, evaluation, and cost planning |
A high-quality adaptive program builds lessons around the student rather than expecting the student to conform to the lesson.
What specialized instruction looks like
This is where the method matters. Data from the Ability KC driving program showed a 100% success rate in participants continuing to drive frequently after training, and that program emphasized breaking tasks into micro-steps, using repetition, and adapting communication for specific impairments (Ability KC disabled driver training).
That doesn't mean every student will have the same outcome. It does show what quality instruction tends to include.
For example:
- For an autistic teen: The instructor may preview every step before the car moves, use highly predictable lesson routines, and practice the same route until scanning and steering become more automatic.
- For a teen with hearing differences: Visual cueing and written reinforcement may matter more than spoken correction alone.
- For a teen with limited leg function: The program should know how to teach with hand controls or other equipment, not just mention them.
Questions to ask before you enroll
A short intake call can tell you a lot. Ask direct questions.
- What diagnoses or support needs do you regularly teach?
- Do you work with occupational therapists or driver rehabilitation specialists?
- How do you handle anxiety, shutdowns, or overstimulation during lessons?
- Can you assess adaptive equipment needs, or only teach once equipment is installed?
- How do you document progress?
If a program says, “We treat every student the same,” that's usually not a strength in this setting.
In metro Atlanta, families often look for hospital-based or rehab-connected services because those settings are more likely to understand the overlap between medical history, cognition, and vehicle control. A center such as Shepherd Center is often part of the conversation locally because families want clinicians, not just instructors, involved in the decision-making.
Vehicle Modifications and Funding Options
Adaptive equipment is where many parents get overwhelmed. Not because the concept is hard, but because the process is fragmented. One professional evaluates function. Another recommends equipment. Someone else installs it. Then the family has to figure out payment.
That confusion is common. Families often struggle to manage the cost and coverage of modifications such as hand controls or wheelchair lifts, and few resources explain how public programs or vocational services may help fund them, as discussed by Navigate Life Texas on driving and transportation options for young adults with disabilities.
Start with the evaluation, not the equipment catalog
The wrong order is buying equipment first because it “sounds right.” The right order is clinical and on-road evaluation first.
A proper adaptive driving evaluation usually answers four practical questions:
- What movement is limited? Foot use, trunk rotation, grip, vision, endurance, or a combination.
- What function needs replacement or support? Steering, braking, acceleration, transfer, seating, or loading mobility equipment.
- Can the teen learn the equipment safely? Some tools simplify driving. Others add complexity.
- Will the modification fit the vehicle and daily routine? A good setup has to work in parking lots, school pickup lines, workplaces, and medical appointments.
Common modification categories
Not every teen needs a major vehicle conversion. Sometimes the solution is modest. Sometimes it's extensive.
- Hand controls: Often considered when lower-extremity use is limited or inconsistent.
- Pedal extenders or left-foot acceleration setups: Sometimes used when reach or leg use is the issue.
- Steering aids: Helpful when grip, range of motion, or one-handed control is a concern.
- Transfer and seating solutions: Important when entering, positioning in, or exiting the vehicle is the barrier.
- Exterior transport equipment: Relevant if a wheelchair or scooter must travel with the driver.
The best equipment is the minimum setup that safely meets the driver's actual needs. More hardware isn't automatically better.
How Georgia families can pursue funding
Georgia families usually need to build a funding path from several directions. That can include medical documentation, vocational goals, school transition planning, and nonprofit assistance. In practice, these are often the most productive avenues to explore:
- Georgia Vocational Rehabilitation Agency: Especially relevant when driving supports education, training, or employment goals.
- Medicaid waiver pathways or related disability supports: Coverage can be limited and highly program-specific, but it's worth asking.
- Condition-specific nonprofits and grant programs: Some help with equipment, mobility access, or transportation-related needs.
- Manufacturer and dealer incentives: For families pricing exterior lifts or similar equipment, it helps to compare automobile lift carrier rebate programs before making a purchase.
Bring the evaluator's written recommendations into every funding conversation. Families get farther when they present a documented functional need, not a general request for help.
Keep copies of every prescription, evaluation summary, installer quote, and vocational justification letter. The administrative side is tedious, but organized paperwork often makes the difference.
Navigating Georgia DDS Rules and Legal Rights
At some point, the process moves from clinical judgment to state procedure. That shift can make families nervous, especially if a teen has a medical condition, a neurological history, or visible adaptive equipment.

Georgia's Department of Driver Services is concerned with public safety. Families should be concerned with the same thing. Trouble usually starts when people approach DDS reactively instead of proactively.
Medical review is a process, not a punishment
If a teen has a condition that affects driving, DDS may require medical documentation. That doesn't mean the teen is disqualified. It means the state wants current information from the treating provider.
The most helpful approach is practical:
- Use treating clinicians who understand daily function, not just diagnosis labels
- Submit complete forms the first time
- Make sure recommendations are specific
- Keep adaptive equipment documentation consistent with the actual vehicle setup
Vague letters create delays. Precise letters help reviewers understand what the teen can do, what restrictions may be appropriate, and what support has already been put in place.
Why tailored coaching matters legally and clinically
The DDS process makes more sense when families understand the range of needs among disabled drivers. A detailed analysis of licensed drivers with disabilities found that physical disabilities were the most common impairment type requiring rehabilitation at 60.34%, followed by brain injuries at 25.56% (PMC analysis of licensed drivers with disabilities). That's one reason one-size-fits-all instruction falls apart. The support has to match the impairment profile.
A teen with limited leg use doesn't need the same training as a teen with slowed processing after brain injury. A teen with strong motor ability but poor hazard judgment doesn't need the same intervention as either of them.
ADA principles still matter
Families also need to understand the difference between reasonable accommodation and lowered safety standards. The ADA supports access. It doesn't remove the requirement to drive safely. In practical terms, that means a teen can seek accommodations, adaptive technology, and individualized evaluation without being entitled to bypass competence.
For parents who want a plain-language overview of those protections in education and related settings, this Parents' guide to ADA and Section 504 is a useful companion read.
Georgia-specific road rules still apply to every beginner driver, so parents mentoring practice sessions should review current driving laws in Georgia and make sure they're coaching from the actual rulebook, not memory.
Your Plan for Practice and Long-Term Success
Once the evaluations are done, the right program is chosen, and any equipment questions are clearer, daily practice becomes the primary driver of progress. Families often think practice means “more hours in the car.” It often means something narrower and smarter.
The most successful home practice plans are repetitive, boring in a good way, and carefully staged. One skill at a time. One environment at a time. One predictable routine at a time.
Build practice around stability
Start with the setting that produces the most regulation and the least overload. For one teen that might be an empty church parking lot in the morning. For another it may be the same neighborhood loop every Saturday afternoon.
Use a sequence like this:
- Vehicle routine first: Seating, mirrors, belt, adaptive equipment check, ignition, brake hold, and verbal plan before moving.
- Low-demand movement next: Straight paths, controlled turns, smooth stops, parking lot lane tracking.
- Add one complexity at a time: Backing, traffic entry, lane changes, parking, then denser road environments.
- Keep the route predictable: Familiarity lowers cognitive load and frees up attention for actual driving tasks.
The lesson should be small enough that your teen can finish it feeling organized, not flooded.
Correct less, cue better
Parents often overtalk in the car. The teen gets a stream of warnings, corrections, reminders, and second-by-second commentary. That usually hurts performance.
Try shorter cueing:
| Instead of saying | Try saying |
|---|---|
| “Watch the speed, check the mirror, turn a little more, stay centered” | “Eyes up.” |
| “You're getting too close to the line and you need to slow down before the turn” | “Slow, then turn.” |
| “You missed that car coming from the right” | “Scan right.” |
Short cues work better because they don't compete with the teen's own processing load.
Think beyond the road test
The road test matters, but long-term success depends on whether the driver can manage real life. That includes planning routes, coping with detours, handling frustration, and knowing when not to drive.
Good long-term habits include:
- Practicing cancellation: If the teen is dysregulated, fatigued, or medically off baseline, the answer is no driving that day.
- Reviewing each lesson briefly: What went well, what felt hard, and what the next session should repeat.
- Revisiting hazard perception regularly: New drivers need continued work on anticipation, not just vehicle control.
Families in Georgia often overlook one useful final step. A defensive driving course can sharpen hazard recognition, reinforce safer decision-making, and help parents become better in-car coaches as well.
Georgia families who want a structured next step can explore Georgia DUI Schools defensive driving courses. The program offers online, live virtual, and classroom options, which makes it a practical add-on for new drivers building judgment, hazard awareness, and safer long-term habits.